Risk of COVID-19 Resurgence
Event date
Speaker
- President, Anthropos Initiative
Presider
 Vice President for National Program and Outreach, Council on Foreign Relations
Vice President for National Program and Outreach, Council on Foreign Relations
From State And Local Webinars.
Laurie Garrett, science journalist, author, and former senior fellow for global health at the Council on Foreign Relations, discusses the implications of reopening states for a second wave of COVID-19 cases.
FASKIANOS: And good afternoon, and welcome to all of you, to the State and Local Officials Webinar, brought to you by the Council on Foreign Relations. I’m Irina Faskianos, vice president for the National Program and Outreach here.
We’re delighted to have participants from forty-nine states joining us for today’s discussion, which is on the record. As you know, CFR is an independent and nonpartisan membership organization, think tank, and publisher of Foreign Affairs, and we focus on U.S. foreign policy. Through our State and Local Officials Initiative we serve as a resource on international issues affecting the priorities and agendas of state and local governments by providing analysis on a wide range of policy topics. Thank you all for taking the time to be with us today. We know that many of you are on the frontlines of responding to COVID-19 in your communities, and we thank you for all that you are doing.
We are pleased to have with us a colleague and friend, Laurie Garrett. We shared her full bio prior to the call, so just—I’ll give you a few highlights of her distinguished background. She is a science journalist and author. She was awarded the Pulitzer Prize for explanatory journalism in 1996 for a series of pieces published in Newsday on the Ebola virus outbreak in the Democratic Republic of Congo. She was previously a fellow at the Council on Foreign Relations, as well as a fellow with the Harvard School of Public Health, where she worked closely with the Emerging Diseases Group. And she’s the author of numerous books, including The Coming Plague: Newly Emerging Diseases and a World Out of Balance. She is a member of many organizations, the World Economic Forum’s Global Health Security Advisory Board, the National Association for Science Writers, and the Council on Foreign Relations.
So, Laurie, thanks very much for being with us today and bringing your expertise to this conversation. I thought, you could talk to us a little bit about the status of the COVID-19 pandemic and what you see as the risks of subsequent waves of infections as the states are beginning to reopen.
GARRETT: Thanks, Irina. And hello to everybody on the call, and on Zoom, and whether you’re with me in audio or visual I will apologize out the outset that there is some sort of police action going on outside my apartment and you may hear very loud helicopters soaring back and forth. Nothing I can do about it.
So if I may, I’m going to go straight to sharing the screen and I’m going to take you through a PowerPoint presentation. Are we—are you seeing it? Excuse me, did it work?
FASKIANOS: Not yet. If you could just try sharing one more time, Laurie.
GARRETT: Let’s see. Let me try again. Share the screen. And here we go. And hello.
FASKIANOS: Now we see it.
GARRETT: Yeah. So, obviously, the issue on everybody’s mind as we’re going into Memorial Day weekend is, can we reopen? What does reopening look like? How do we do it? What are the risks? And we have not received consistent guidelines from the federal government that really tell every single state some consistent policy of the new CDC guidance that was released earlier this week. Let’s just say they put the burden back to the state repeatedly, and sidestep a lot of the very specific questions that I’m sure are on your minds like, do I have to test everybody? Who do I have to test? With what tests? And when, and how, and with what frequency?
So let’s just remember where we were back in March 1, when the first projections were made about where our epidemic was headed. And at that time, it looked like the upper limit was going to be ten million people dying in the United States, perhaps even more. This was assuming that we didn’t go on lockdown, we didn’t shut down America, and we didn’t take the great economic burdens that we have suffered. But of course, we went in another direction. Many states went on lockdown beginning in March. And on April 16, the White House issued its guidelines for what barriers or gating should be achieved in order to open up again. The phase one openings, for example, called for very specific kinds of activities still limited, other activities allowed. But as you can see, the language was not specific. This was as specific as it got.
Again, it threw the burden of teasing these points out to the states, and to employers, suggesting that they use some kinds of testing, but no specifics on when, and how, and where. Some kind of temperature checks but, again, no specifics. And phase two pretty much said: It’s up to you, states and regions. You decide what your phase two will be, what the gating criteria will be, and how you will execute it. Phase three, for both individuals and employers, put a pretty tough burden on the respective individuals and entities, the organizations, to make their own decisions and their own kind of calculus of what would be an appropriate algorithm for safe reopening and getting the economy rolling again.
And as far as core preparedness responsibilities it was, as I’ve said several times, entirely really put on the states, and how the states would work with their municipalities which, as we have seen, has unfolded to be a tense relationship in many states, with cities taking one set of policies, the states taking another, protests leveled at tiers of structure for governments.
Well, at that time, we also had a very wide range of forecasts of what might be the trajectory for the American epidemic, with Imperial College out of London giving the grimmest forecast and probably the most optimistic was the International Health Metrics and Evaluation Group at University of Washington. That, perhaps not surprisingly, became the key go-to group for the White House. But you’ll notice that at that time the reported levels were already very much mirroring the actual trajectories proposed by Imperial College. And that is the reported cumulative totals put together every day by Johns Hopkins University.
If you looked at those models, you could see future death burdens across a wide range of estimates, but none of them looked particularly good. Any way we looked at it, New York City in particular, and state, were facing a very grim future, if severe lockdown didn’t go into place. It’s been in place now for quite a while. And the result has been a rising level of anger from what turns out, according to polling results, to be a small minority in American public opinion, certainly less than 20 percent of Americans, but nevertheless a very active and very loud one reflecting a lot of the economic pressure that the lockdown is bringing on every single state and municipality across the country.
On May 17, HHS Secretary Azar said that it looked like everything was going gangbusters, that the spikings were not occurring where states had started to open up, and in particular Georgia had started opening up, and Texas, by this time. And it seemed that the overall net trajectory for the nation was quite promising, a downward trend. It was safe to look towards Memorial Day weekend as a big end of lockdown reopening period. So where are we after that time?
Well, one key point that was missed right from the beginning is what it meant that New York City, New York state, Detroit, and New Orleans constituted the majority of the totality of cases of COVID-19. If you look them out of the equation of measuring where was the United States at that snapshot moment, as it turns out the U.S. was on a terrible trajectory, that what you were seeing as a downward trend was really a reflection of the success of the lockdowns in New York, Detroit, and New Orleans. If you took those big numbers out of the equation, suddenly the United States didn’t look ready to get out of lockdown at all.
And if you added in the undercount of COVID deaths, the burden of deaths that has surely been the case everywhere in the entire world, in fact, not just restricted to the United States or to any given part of the United States, you could see that actually we were facing a far grimmer view of our epidemic than the official count would seem to tell us. And that’s because there was certainly a big, excess, overall mortality going on, but we weren’t testing everybody that died. Many people died at home or in non-hospital facilities. And the overall guesstimate of what mortality looked like in the United States was greater underappreciated. Excess all-cause mortality seriously skyrocketed in late March and into mid-April all across the United States. And these certainly were not counted totally as COVID deaths.
Across the world, we see a similar trend, where there’s been a great undercount of the scope, and size, and scale of this COVID disaster. It you look particularly at the United Kingdom, Italy, and Spain, you can see big spikes in overall deaths compared to their historical average. So the historical average is the blue line and the spike is the red line. And you can begin to see just how profound the differential has been. In New York City, it was really, really dramatic. And not—a very small percentage of that has been counted officially as COVID.
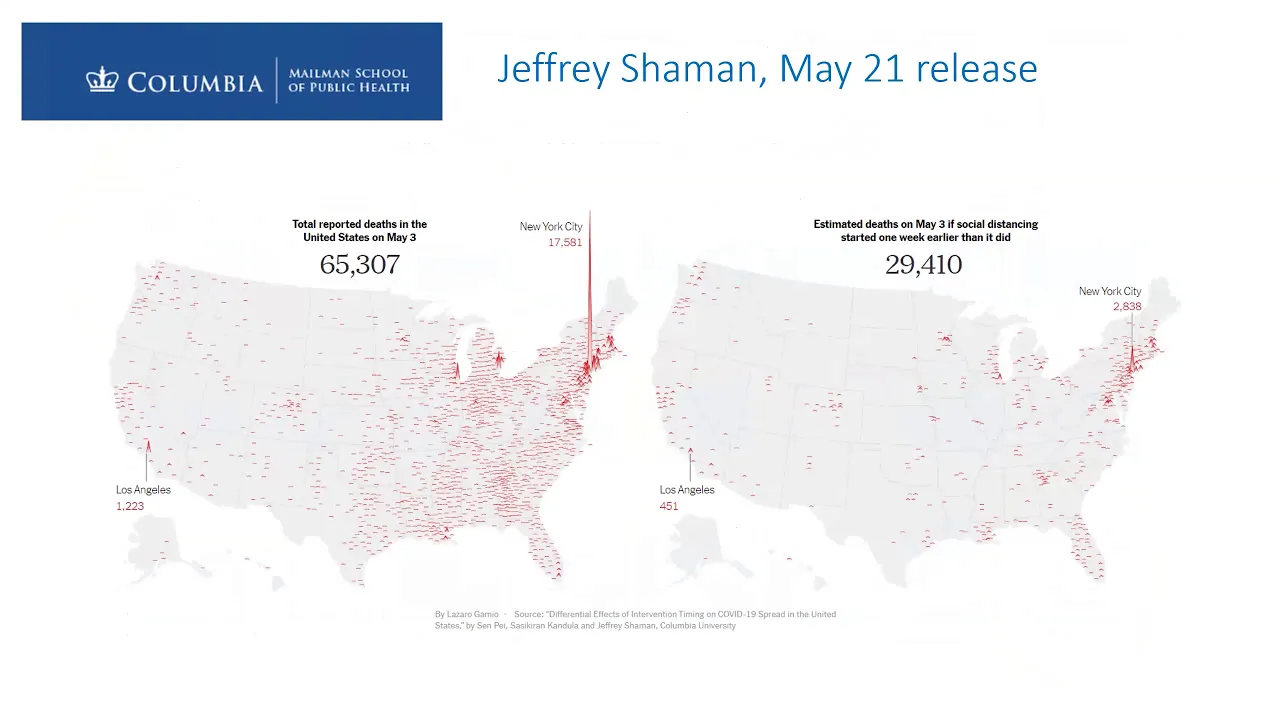
Jeffrey Shaman just released yesterday—and you’ve no doubt heard about it—from Columbia University a very startling estimate of what just simply having started our lockdown one week earlier would have meant in terms of lived saved. If the lockdown had gone two weeks earlier, started in the first week of March instead of as was the case in most places well after St. Patrick’s Day, we would have saved some sixty-five thousand lives nationally and thirty thousand in New York area. And that, obviously, has ramifications for how we anticipate what we’re doing now. If we reopen too fast it would be like starting too late in the first place.
And we would see, particularly in the tri-state area of New York, New Jersey, and Connecticut, perhaps a mirroring of what happened back in early March, with this skyrocket—if you look to the gray, that is the period of lockdown, the dark gray, when you see cumulative death tolls that are enormous, but they most reflect infections that took place before the lockdown went into place. Now where are we? And do we actually have standards met that say it’s safe to reopen, it’s safe to bring America back to full operation, or some sort of scale of operation that includes things like opening up hair salons, bars, restaurants, core businesses, travel, and so on?
Well, one of the criteria set down by the World Health Organization is a consistent below 5 percent zero positivity rate. Meaning, you’re testing, you know what your rate of infection is of new cases, new infections. And you are consistently finding rates that are below 5 percent. Well, as it turns out, most of America’s states have not met that criteria. Twenty-six have failed to keep their levels below 5 percent. And Puerto Rico was at 100 percent. So this is not looking promising. If this is going to be your criteria for opening, it means it’s too soon to open right now.
Imperial College just yesterday released a very startling report. And what it does is attempt to take the European standards, particularly the German standard as laid out by Angela Merkel for reopening and apply it to the United States. So what is that? They look at the R0, which I don’t need to tell most of you on this call but just for the handful that might not be familiar, an R0 is a measure of the rate of reproduction of an epidemic. And it’s a statistical measure that says: If I, Laurie Garrett, am infected, I am statistically likely to infect how many more people in the time that I am contagious? One? Two? Ten?
We know in early-stage New York the R0 was five, which means that we—the epidemic was increasing fivefold in a very high pace from one step, to another step, to another step. A horrible, horrible rate of increase. And under the German model, and consistently adhered to across most of Europe, the goal is to achieve an R0 of below one, so that you’re shrinking your epidemic over time. In other words I would, Laurie Garrett, infect less than statistically one person during the time that I am contagious.
If you look at this analysis released yesterday by Imperial College, the majority of the United States has not yet achieved an R0 of one or less. New York has, which is good news. And a few key states that already had low R0s to begin with have managed to succeed. But some of the states that are opening very rapidly, such as Texas, Arizona, Georgia, and the key southern states, and of course states in the industrial Midwest, have definitely not even come close. The probability that they have achieved an R0 is below 25 percent. That would argue that it would be a very bad idea to be opening wildly in most of these states.
And this is the Imperial College estimate put out yesterday of the rates of infection—the total percentage of the population likely to have been infected as of May 17 in key states. Now this is important because many have argued that, well, we should just do the Swedish model, aimed to achieve a herd immunity, and let the virus flow while keeping the economy open. Well, herd immunity you would want to be up in the ballpark of 90 percent of your population has been exposed and developed antibodies. What this study estimates is that nationally we’re at about 4.1 percent, have tested or would best positive. Montana is at a low of less than 1 percent, 0.2 percent. New York is the highest at 16.6 percent. So despite our devastating epidemic here in the tri-state area, none of the three states have achieved anything remotely close to herd immunity, of course.
So this leaves a lot of scientists to be very fearful that a rush to reopen is going to lead to a second surge of this entire epidemic. And not a surge off in the distant fall, but quite immediately—perhaps in July or even late June. And there are some special concerns that are brought to bear. First of all, several states, if you look for just have you met the gating criteria set out way back in April by the White House, you can see that most of the states have not. And they’re trending in the opposition direction from what even the White House gating criteria of April was. Nursing homes have proven to be horrible, tragic breeding grounds for COVID-19 spread. And we’ve seen outbreaks in almost every big center of nursing home populations across the nation. It continues to be very difficult to maintain safety for the housed population and for their staff.
Similarly, meatpacking operations and food prep processing plants have had explosive outbreaks all across the country. And in many counties, particularly in North and South Dakota, in Minnesota, in Iowa, Indiana, we see that the meatpacking plant is the source of up to 90-plus percent of all contagion in the county and the number-one cause of spread and burden on the county health system. We also see a very disproportionate burden of deaths in counties that are heavily populated by African American and Latino populations versus white populations. So the highest death tolls are consistently in counties with high African American populations. And while there are many reasons given for this, none has been specifically highlighted as the key concern, although hypertension is the one clinical marker that seems to track with 100 percent of COVID deaths. And hypertension is, of course, much higher in the African American population compared to white population.
There is a rising distrust of testing data and of overall reported deaths and other data in several states. This leads to a kind of public distrust of the what the government is telling them about the safety of reopening. Georgia, Florida, Texas, Vermont, and Virginia have specifically been highlighted in a number of reports for some suspicion of the reliability of available data. In Florida, there’s the notorious case of Rebekah Jones, who was the lead scientist in charge of Florida’s system of reporting. She was told, she says, to manipulate COVID-19 data in order to accommodate a positive image of the lockdown results, or the reopening—the ending of lockdown. She says she was fired. The state says otherwise. Stay tuned for more.
Meanwhile, the Florida Medical Examiner’s database has been closed from public view. It was shut down, no longer can it be viewed, but it was already starting to show some very dangerous trends, especially associated with people with underlying chronic disease problems—diabetes, hypertension at the top of the list. Just this week the CDC released a major report and analysis of spread within a specific church population in Arkansas as a cautionary tale. This actually took place in early March, but it is demonstrative of what many people at the local level fear could happen with an overly rapid reopening and returns of congregations of all faiths to a sort of pre-COVID level of gathering and activities related to their religious faiths.
And while everybody would like to have the communalism restored and the sense of support in all of these church settings, this is really a cautionary tale. I mean, a third of the church population acquired COVID-19 as a result of attending the church. And it killed three of them. That’s tragedy compounded many times over. And in New York, while we are declaring victory—or, at least the governor is—and saying that great things have been achieved with these tough COVID lockdown standards, it should be remembered that what we have basically achieved is getting back to the level we were at when things stated to skyrocket, which is hardly a level of safety given that what ensued when we were at that level back in early March. So we are still a long way from being at a level that would allow everyone to feel quite safe about returning to the office, returning to restaurants, and so on.
And a big cautionary tale out of China. After the toughest lockdowns any nation has executed, with the possible exception of the lockdown procedures in Italy, China has now seen a resurgence in at least two different parts of the country and one hundred million people have been put back in lockdown this week as a result. Though, interestingly, the People’s National Party Congress is underway. It’s in its third day today in Beijing. And as far as I’ve been able to hear, there’s not been any mention of this whatsoever in any of the proceedings.
So with that, I will exit the sharing—screen sharing, if I can figure out how to do so, and—or, you can exit my screen sharing from your end. And I’m happy to take questions and hear from the many people participating today.
FASKIANOS: Fantastic. Thank you so much, Laurie. That was really a great and upsetting overview. And the PowerPoint really helped bring it to life, to see how it’s—the graphics of it.
(Gives queuing instructions.)
In addition to asking your question, we encourage you to share, you know, best practices in your community. And for both Laurie and my sake, and all of our—the entire group, please say your name and identify who you are and what state. So it just helps with context and helps—will help Laurie give a better—a more focused answer.
So let’s first go to Raphaël Debraine.
Q: Hi. My name is Raphaël. I’m with the Lieutenant Governor’s Office in Virginia.
I was just quickly wondering if I could get—or, if we can all get a copy of the data you provided, those slides, because it has a lot of useful information that I know my office would love to see.
GARRETT: Well, that’s up to Irina. She’s got it now. (Laughs.)
FASKIANOS: And as long as Laurie says it’s OK we will share it out with this group, because it really is a fantastic presentation.
Q: Yes. Thank you very much.
FASKIANOS: Thank you, Raphaël.
Let’s go to Emma Pinter.
Q: Thank you for that. My name is Emma Pinter. I am the chair of the Adams County Commission in Adams County, Colorado.
And so we’ve been on the frontlines of COVID response. We have a rather large Hispanic population. Under the age of twenty-five are 56 percent Hispanic. But over the age of twenty-five are about 40 percent. And we’ve seen similar impacts like you described in your slides. One of the questions that we have been really wrestling with is, yes, there are hypertension and other health issues regarding the disproportionate impacts of COVID in Hispanic and Black populations, but also we found that those populations tend to have frontline worker jobs. And we have had a really hard time parsing out that data. Is this an economic justice challenge where folks of a certain community are more likely to have a frontline worker job? Or is it biological and health-related? And if you had any thoughts or guidance on that topic, I would be really interested in hearing it.
GARRETT: I do. And I think that it’s a fundamental question. It’s one that everybody’s wrestling with right now. There’s a brand-new report just out I think today. I read so much, it’s like a firehose, you know, of data pouring in these days. But there’s a new study that looks at health care workers’ seroprevalence compared to the general population in the United States. And it’s quite startling that despite their daily exposure, health care workers actually have a lower level of seroprevalence compared to the general population in their respective communities. So that tells you that with the right protective gear you actually do dramatically reduce your risk of acquiring COVID. It also tells you that if those frontline workers that are doing things like making food deliveries, and handling sewage and sanitation, and farm work, and so on, are appropriately protected with the right PPE, that should greatly cut the risk for them.
But there, I think, is a second thing to consider, and that is that, you know, we know the virus uses the ACE2 receptor in order to gain entry into cells, whether the cells are in your lungs or elsewhere in the human body, and particularly the kidneys and throughout the cardiovascular system. And we know that there’s a very diverse level of effects that this darn virus has on the body. We’re just now appreciating how great the burden is as a pediatric syndrome the mirrors Kawasaki syndrome. And so all of this put together tells us we’re dealing with a real monster here, but it’s a monster that has one specific receptor. It needs to have access to, that ACE2 receptor.
And of course, the key thing about the ACE2 receptor is that it’s all about angiotensin and it ultimately regulates the cardiovascular system, your heart rate, and blood pressure, and so on. And so there’s such a deep relationship between the ACE2 receptor and hypertension that I am—I, for one, feel very strongly that health departments should as a side-by-side tandem effort with general COVID testing be administering basic blood pressure workups. Since they cost nothing, just slap the cuff on and, you know, you can train nonmedical personnel in how to listen for the blood pressure markings, and then perhaps add to it, you know, a handy-dandy pulse oximeter in order to test further what the heartrate and oxygen uptake is.
These are so cheap to do, so quick to do, they’re noninvasive, they can be administered by people without really advanced medical training of any kind. Why not do it? Why not make it a consistent part of all COVID testing, so that you begin to offer the would-be client a double whammy. One, we’re going to let you know whether or not you’re infected, or if you’re doing antibody tests whether you historically were infected with COVID. But we’re also going to tell you if you are at risk, a special risk, if you get COVID of going into dire medical outcome and potential death. We’re going to tell you that. And add to it, we’re going to help you get services to deal with it because they’re so cheap, and the cost-benefit ratio, to my mind, is highly in favor of the states spending on that intervention versus what it will cost to treat them for acute COVID—put them on a ventilator and possibly face mortality.
And so if—you know, imagine if the Latino population in Colorado is not only getting COVID tested, but they’re getting a blood pressure workup at the same time, and they’re finding out if their heartrate is too high, or if they have low oxygen uptake because of other underlying conditions. And then they’re being referred for free treatment. Put them on hypertension medication. Get them in the kind of care that can lead to lowering their overall risk and helping us to answer the puzzle you asked. Are these people dying because of their underlying biological susceptibility? Or are they dying because they’re more likely to be exposed? One, the solution is better PPE for them. The other, the solution is let’s deal with their underlying health condition.
FASKIANOS: Thank you. Let’s go to Senator Karen Keiser. OK. You’re unmuted. Go ahead.
Q: Well, thank you very much. Thank you so much for this presentation.
I am—one of the jobs I do in Washington state is the chair of the Labor Committee. And I’m trying to figure out how we connect the dots between essential workers and their employers and the preparations and prevention steps that we can take. We’re looking at meatpacking plants, food processing plants, grocery workers, nursing home staff—all of these sort of hotspots where we really have very good knowledge there’s a higher risk of infection, but the employers do not report the cases based on their employees. We only get the cases through our Department of Health, not through our Labor Departments. And we don’t connect the dots. It’s a puzzle. I’m trying to fit the pieces together. Do you have any advice for that?
GARRETT: Well, I’m not an expert in that area, but one thing I would suggest is that a lot of the regulations, particularly for all the health settings—or, the job settings you described, a lot of the regulations are set down by OSHA at the federal level and NIOSH, and then OSHA and NIOSH equivalents at the state level. And there is the capacity to enforce. It varies state by state, and I’m not familiar with the Washington state law, but I would imagine that, you know, it’s very hard for the health department in many states to have the legal right to do unwelcomed site inspection. You know, they have to sort of notify ahead of time they’re coming. You never know if you’re seeing the workplace the way it really is, or you’re seeing it spiffed up for the visit.
Q: But our state labor agencies have that right and they have that standard.
GARRETT: Exactly. Exactly.
Q: So that’s why connecting—
GARRETT: That’s where I was headed.
Q: OK.
GARRETT: That’s where I was headed, Senator, because that’s exactly the point. The legal right, the clout, to march in without advance permission, and to see on site, and to take reports on a confidential basis from the labor force, those rights are in the hands of OSHA and OSHA-equivalents at the state level. And if they are very clear about what they are supposed to be looking for, which I think is really important—you don’t march in, look around, and go, I don’t know. I think it’s crucial to know: What are the PPE you expect staff to have? What are the—what’s the nature of risk in those settings? And what sorts of mitigation should be taken and are a burden of the employer? And then do that level of inspection.
Q: Thank you.
FASKIANOS: Thank you.
Gerald Sonnenfeld.
Q: Hello. My name is Gerald Sonnenfeld. I’m the retired vice president for research—
GARRETT: Gerald muted.
FASKIANOS: Gerald muted.
GARRETT: We lost him.
Q: Can you hear me now?
FASKIANOS: Yes, we can.
Q: OK, good. I’m Gerald Sonnenfeld. I’m the retired vice president for research and economic development at the University of Rhode Island. So I now live in Arizona. I’m also an infectious disease immunologist. So if I were still working, I imagine I’d be pretty busy right now.
My question is, since there are questions with the validity of the PCR test for—that’s used to detect virus and of most of the antibody tests, how valid are any of the data that we’re receiving, even if they are not all bad?
GARRETT: So really important question that you’re asking, and I’m glad you asked it because I didn’t have time to put it in the PowerPoint. As you say, there are problems with many of the tests available, both the antigen tests, the antibody tests, and the nucleic acid test. So just for the sake of anybody on the call that doesn’t know the difference between these, let me just point out that the nucleic acid tests, if they’re working properly, give you one answer. And that is: This human at this moment that blood was drawn, or saliva, or a nasal swab—at that moment the person was infected with virus. If the antibody test is working properly, it’s telling you at some time since this COVID-19 SARS-CoV-2 virus appeared on planet Earth, this individual was infected and has made antibodies against it, which we are now measuring. Or if it’s an antigen test it’s not even measuring antibodies. It’s saying this person has some evidence of having had the virus in their body at some point.
All three are important things to know, not about every individual but to know for public health purposes. And only the nucleic acid one is particularly useful as a diagnostic in a medical setting. All three are useful in different ways for public health tools, to guide policy, to help governors know what have I got here in the state, to help mayors know which neighborhood is getting the most new cases, and that sort of thing. But they are all flawed. And in this rush to produce test kits we’ve seen a lot of fraudulent, to put it bluntly, things hit the market. And then we’ve seen a lot of really great tests, like a couple of new very promising CRISPR-based tests never even getting bankrolled to hit the market at all, so they’re just not available.
I think the really big cautionary tale here is what happened in South Korea. South Koreans unfolded with massive testing. It has had a huge impact on their capacity to bring their epidemic under control. And overall, the net benefit far outweighs any cost in terms of the scale and utility of their mass testing. It was key to bringing it under control in South Korea. But they did see, they thought, quite a large number of people who tested negative twice, were released from hospital or from whatever facilities they were in, an told: You’re healthy. You’re over COVID. You’re OK. And then either showed up sick later or tested positive in a subsequent test. And we now know, both in China and in South Korea, a lot of the later tests positive turned out to be fragments of dead virus. So the nucleic acid tests were actually overly sensitive and gave false-positive results.
I personally think I’d rather have false positives than false negatives, but that’s up to you to decide. I would say at this point we don’t really have good protocols for how to use any of the three tests for public health purposes. We don’t have tests developed with the right level of sensitivity and specificity. The FDA has approved, I believe, the last I looked, ten antibody tests. I could be wrong. Haven’t looked today. And definitely most who have independently looked at the antibody tests have said the majority stink. They’re really lousy. So we have a long ways to go to get better quality, not just quantity, of tests.
FASKIANOS: Thank you.
Representative David Tarnas.
Q: Thank you very much for presenting today.
I live and work in Hawaii. And we have great health metrics right now with our virus. We are slowly reopening our local economy. But we for travelers are requiring a fourteen-day quarantine. That has reduced our visitors by 90-plus percent. There are very, very few coming in. We are struggling economically because we have a primarily tourism-based economy. So we need to reopen. Everyone’s pushing for some kind of protocol for doing that—testing visitors—testing travelers before they leave their point of demarcation. And yet, I worry about the efficacy of the testing, methodologies, technology. FAA has said we can require it, but do you think that we can actually set up a protocol that would be effective? So we’re really stuck. We need to open our economy to visitors. We’d like to get rid of the fourteen-day quarantine. But we don’t want to expose our residents to the virus again. So any suggestions?
GARRETT: Well, aloha. And mahalo for your question. I would suggest that you not look to the mainland for answers to your questions, and instead look to New Zealand. If there is a success story out there with COVID, it’s New Zealand. It’s extraordinary how much they have almost completely eliminated COVID risk and yet, like you, they are very dependent on tourism. And of course, as an island nation, they are, like you as an island state, dependent on frequent movement between themselves and the rest of the world for trade, for their supply chain, for food, everything. And I think that a close study of what have been the measures implemented in New Zealand would likely offer you some sound advice.
Specifically on things like how do you work with the airlines to ensure that passengers are not carrying COVID, and that you don’t need to bring them under a fourteen-day quarantine, and that sort of thing? I would say that’s beyond my personal expertise, and I would urge you to instead look and speak with your counterparts in New Zealand.
FASKIANOS: Thank you.
Let’s go next to Commissioner Daniella Levine Cava.
Q: (Off mic)—much. What an outstanding presentation. I’m county commissioner in Miami-Dade County. And so we are another hotspot here. And we have been coming down in certain indicators. And what has recently been happening in terms of measuring the impact is an effort by our mayor to distinguish or to separate the nursing home related cases. And while obviously that is an area that is growing at a higher rate than others, I wonder your thoughts about that kind of segregated measurement. You know, whether—it’s good to know, but does it in any way suggest that we’re doing better with our containment efforts? Or basically, how should we read that, if we can look at specific populations that are more sequestered to see that they are the ones really growing?
GARRETT: Thanks, Commissioner.
I would say, first of all, most people in epidemiology, most people in public health would tell you the most disaggregated your data is, the more useful it is. If we can find ways to tease out trends down to the smallest, most minute level, there are more identified ways of intervening. We get more sense of pattern and who’s at risk and who’s not at risk. But of course, the problem is when highly disaggregated data goes public, there’s always the risk that certain people will see it through their political and cultural prism. An example might be if you are in a city where disaggregated data reveals that an excess of 50 percent of the deaths are in African Americans, the majority white population might become dismissive of the epidemic, might come to believe, well, it’s not my problem, and that somehow the virus knows your skin color.
Similarly, in communities where a very high percentage of the at-risk population turns out to be in nursing homes, a lot of young adults in particular tend to then pooh-pooh the risk for themselves and to think, well, it’s just a problem for old people. And I, as a healthy, vibrant, jogging thirty-two-year-old have no risk. And then they may be more likely to carry out activities that, indeed, would put them at risk for exposure. We’ve seen that very problem that just described here in New York City.
But from a policy point of view, the disaggregation is absolutely essential. So I would say, if there’s a problem there it is a communications problem, which is to say you need disaggregated data. The mayor is probably right that he needs to understand what percentage of the burden of Miami-Dade or Miami city infections are about your senior population, and particularly your cohoused population. And that has—that tells you where to direct resources, and direct personnel, how to bring it under control, where you need to really target your innovations. But the communications burden is on a whole different part of the government, and including the mayor, to make it very clear to the general population: Just because we’re seeing a higher, you know, maybe 40—I’m making the number up—40 percent of the cases in Miami are from the nursing home setting, that doesn’t mean that the remaining 60 percent is no big deal, or that you have no risk at all in your life. So I would say it’s really more of a challenge of effectively communicating how risk parses out than it is a reason to not disaggregate the data.
FASKIANOS: Thank you.
Let’s got to Mayor Curt Leng.
Q: Good afternoon and thank you so much for taking the call. I’m the mayor of a town that is a suburb of the city of New Haven in Connecticut. We have sixty-two thousand people. And your information was so very informative and helpful.
I’d like to just throw out a couple of quick questions to get your thoughts. I feel in general, and I’d like to see if you agree, that Connecticut is being very cautious and slow with the reopening process. However, I think that there’s more that our local governments could be doing. And I need some guidance on what you think might be the most effective steps that we might be able to take, either as local governments or with our local health districts. And then my second question, if I could throw it out there and then I’ll just be quiet and listen, is that the city of New Have and the town of Hamden, my town, were the two communities in our state that did further restrictions in childcare centers. And while I understand the socioeconomic implications of having them closed for people who are trying to get back to work, I’d like to hear your thoughts on opening those childcare centers for—(inaudible)—kids while the schools are still closed.
GARRETT: OK. Well, thank you for that. And greetings in the tri-state area.
First of all, I think one the startling findings—another paper just published in the last two weeks shows that if you look at anti-lockdown sentiment and mobility associated with it—so, for example, protesters that have gone to state capitals to protest lockdowns, or groups of individuals that defy lockdowns to go to events, such as concerts, or church assemblies, or sports events, whatever they may be. It is striking the distances people have traveled to attend such events. In one study just measuring cellphone patterns, the average movement—and this would have been in Texas-Georgia area. The average movement was more than 150 miles. So for example, when Georgia opened up hair salons, people drove from Alabama and from Mississippi to Georgia to get a haircut.
What this says to me is that if one city or locality changes their, you know, regulations and their standards in a way that deviates strongly from other local in the region cities and localities, you may see your population—a substantial number of them—go to that looser spot, that differently regulated spot, or cross a state line, and then return possibly carrying COVID back to your hometown. This means that there’s a real burden on individuals, like yourself, that are the leaders of communities to form strong regional alliances with neighboring communities, and in particular to identify those that you know already, even in pre-COVID times, were the directions of mobility and travel.
For example, if there’s a big Costco, you know, two towns over, and you know that a lot of folks in your town go to that Costco every Saturday, or Sunday, or what have you. Well, then that should be a target for your attention. If there’s a particular direction people go for sporting events, or entertainment events. I imagine in your case a lot of it is heading into New Haven and back out again. And as far as the childcare question, I’m really going to want to boot that to people with greater expertise about specifics of risk in childcare settings.
FASKIANOS: Thank you.
Let’s go to Senator Bob Hasegawa.
And I apologize, we have so many questions in queue and we just not going to get to them. We’re just going to have to have you back, Laurie. (Laughs.)
Q: Thank you so much for taking my question. I have a question about—
FASKIANOS: And you’re in Washington state, correct?
Q: Washington state senator, yes. Thank you.
FASKIANOS: Thank you, Senator.
Q: So a couple quick questions. Does immunities—or, does antibodies, presence of it, suggest that you have an immunity? And secondly, the whole question about droplets versus, like, breath vapor. I’m concerned that by—that—well, the question is obvious, I guess.
GARRETT: Yes, I know where you’re going. (Laughter.)
Q: OK.
GARRETT: OK. So it’s microdroplets and the first one, again, was—
Q: Oh, the first one was about antibodies—
GARRETT: Antibodies! Sorry. I got distracted by the police helicopter out my window again.
FASKIANOS: We haven’t heard it.
GARRETT: So the antibody question is still a very hot potato. There is data in all directions about whether or not the presence of antibodies along constitutes, guarantees that you actually are immune, and your body would muster a strong response in the presence of COVID-19. Part of it is because of something I referred to earlier in response to—who was it—I forget. (Laughs.) Somebody else’s question about the quality of the tests to begin with, and antibody tests in particular we’re having trouble with. The other is, what kind of antibody are you looking for? Are you looking for IgG, IgM, et cetera, which immunoglobulin class, but also are you specifically looking for the presence of neutralizing antibodies?
So, you know, it’s possible to have, for example, as many of you on this call probably have right now, out of control antibodies freaking out about hay fever. And you’re getting your, you know, spring allergies, and coughing, and sneezing, and all of that. But those are not neutralizing antibodies that result in, say, destroying a hay fever dust pod. They are a whole different part of the immune system. And if your immune response to COVID is in one of those other arms of the immune system it’s not going to be a protective immune response that’s there for you the next time COVID comes around. There are—there definitely are neutralizing antibodies in people against COVID that have been conjured when an individual was sick with COVID. And we are increasingly finding people who never had symptoms but do have neutralizing antibodies.
If we hadn’t found any neutralizing antibodies, I don’t think Tony Fauci or any of the other top tier of the NIH would be the least bit optimistic about coming up with a vaccine because, of course, the goal of vaccination is to stimulate the production of neutralizing antibodies. So we do think there are people who muster effective immune responses against this virus. And there is now production of convalescent serum, meaning drawing plasma from individuals who survived COVID on the assumption that they have neutralizing antibodies in their plasma that can help in the treatment of other sick individuals. And there’s quite a robust industrial response in the biotech industry right now in development of immunoglobulin-based treatments that can be used to treat people without having to draw plasma. In other words, they’re artificially generated based on what has been found in plasma samples.
So that’s the answer to that part of the question. And the second was, oh my goodness, I just forgot it again. What was the second part? Oh—
FASKIANOS: Droplets. It was about droplets.
GARRETT: Oh, thank you. Just too much—I’m so distracted. There’s just too much going on. The droplets, yet.
So one thing I would urge everybody to do is to go on your favorite video providing YouTube, or what have you, and go Nokia, N-O-K-I-A, that’s the leading television distributor of Japan. Go Nokia and microdroplets. And you will see a few video recapitulations of droplet exposure done very cleverly using laser beams and so on by folks at Nokia, working together with scientific teams in Tokyo. And it’s pretty persuasive. I mean, you really do see that a cough or even random conversation disperses microdroplets that could be COVID positive over vast distances. And that the micro—the smaller the droplets, the more likely they just simply recirculate in the air in a closed space for a long period of time.
Of course, there’s a one really standard solution to this threat: Open the darn windows. You know, the main reason that we see more contagion, more infection in the winter has nothing to do with temperature. And, you know, unfortunately our president said that come April when it’s warm, the virus will go away. That was a really big misunderstanding of the connection between seasonality and spread of viruses. This virus, of course, prefers a very higher temperature, 98.6, the temperature of your body. That’s where it likes to be. So hot is the issue. The issue is human behavior. When it’s very, very cold outside we close all the windows, we turn the heat up, and we stay indoors. And it’s in those indoor settings without air circulation that virus is most likely to recirculate from one person to another, to linger in the air, and to be on surfaces so that, you know, sharing something like your cellphone might theoretically also mean sharing virus.
But the good news is that we’re now in a season where everybody can open the windows. And if there’s one, you know, great public health recommendation, it would be: open them, and open them wide. Now, what are we—what I am I worried about next? Air conditioning. So we do have two studies that were done in January out of China. Well, one is actually Singapore and the other is southern China, where it was still tropical hot in January. And they found an association between people in a restaurant in one case and a household in the other, and dirty air conditioners. And so one thing I’m a little anxious about is that because of the lockdowns, very few people have had their HVAC systems or their personal air conditioners maintenanced this spring. And this is usually the time of year when everybody’s calling up their air conditioning guy and saying: Come give it a test, check the system, clean it out, what have you.
So we could actually go straight into a heat wave sometime in the next two or three weeks in most of the eastern part of the United States, and certainly the South, and people would be cranking—closing the doors and windows again, going back into enclosed spaces, but with unmaintenanced, dirty air conditioning systems. And that’s a concern.
FASKIANOS: Well, Laurie, thank you very much for this riveting hour. And I apologize to all of you on the call, we could not get to—or, webinar—we couldn’t get to your questions. And we’re just going to reconvene, and we will keep bringing people like Laurie Garrett back to help you sort through these issues. So we will be sharing the audio, and video, and transcript of this webinar with you all soon. You can follow Laurie Garrett on Twitter at @Laurie_Garrett. And you are going to see her regularly on CNN. And, I think, tonight here on NBC. So, Laurie, we will have you back, but thank you for your analysis and information. And we will circulate her PowerPoint presentation.
The next webinar in the series will be on Wednesday May 27 from 3:30 to 4:30 p.m. Eastern time. And we will be talking with Heidi Crebo-Rediker, who’s a senior fellow at the Council, on the future of American infrastructure, given the budget cuts that many states and local governments are facing. So we’ll be sending the invitation out later today. Again, please go to CFR.org, ThinkGlobalHealth.org, and ForeignAffairs.com for the latest analysis on COVID-19. And, as always, please share your thoughts of how we can be of help by sending an email to [email protected]. So stay well, stay safe, and thank you, again, Laurie Garrett.
(END)



